
Alcohol Dependence Medication Comparison Tool
This tool compares key aspects of Disulfiram (Antabuse) with other commonly prescribed medications for alcohol use disorder. Select a medication to see detailed information.
Disulfiram (Antabuse)
Aversive conditioning medication
Naltrexone
Opioid antagonist
Acamprosate
Neurotransmitter stabilizer
Topiramate
Anti-seizure medication
Gabapentin
Anti-seizure medication
Baclofen
Muscle relaxant
Effectiveness Comparison
Abstinence Rates
Side Effect Profile
When you or a loved one is trying to quit drinking, the medication choice can feel like a maze. Disulfiram is better known by its brand name Antabuse and works by making alcohol taste terrible. But it isn’t the only option on the market. Below you’ll find a side‑by‑side look at Disulfiram and the most common alternatives, so you can decide which drug (if any) fits your lifestyle and health profile.
Key Takeaways
- Disulfiram creates an immediate aversive reaction to alcohol, while other drugs aim to reduce cravings or block alcohol's rewarding effects.
- Side‑effect profiles differ: Disulfiram can cause severe liver toxicity, whereas Naltrexone may trigger headaches and nausea.
- Choosing the right medication depends on liver health, motivation level, desire for strict abstinence, and whether you can tolerate daily pills.
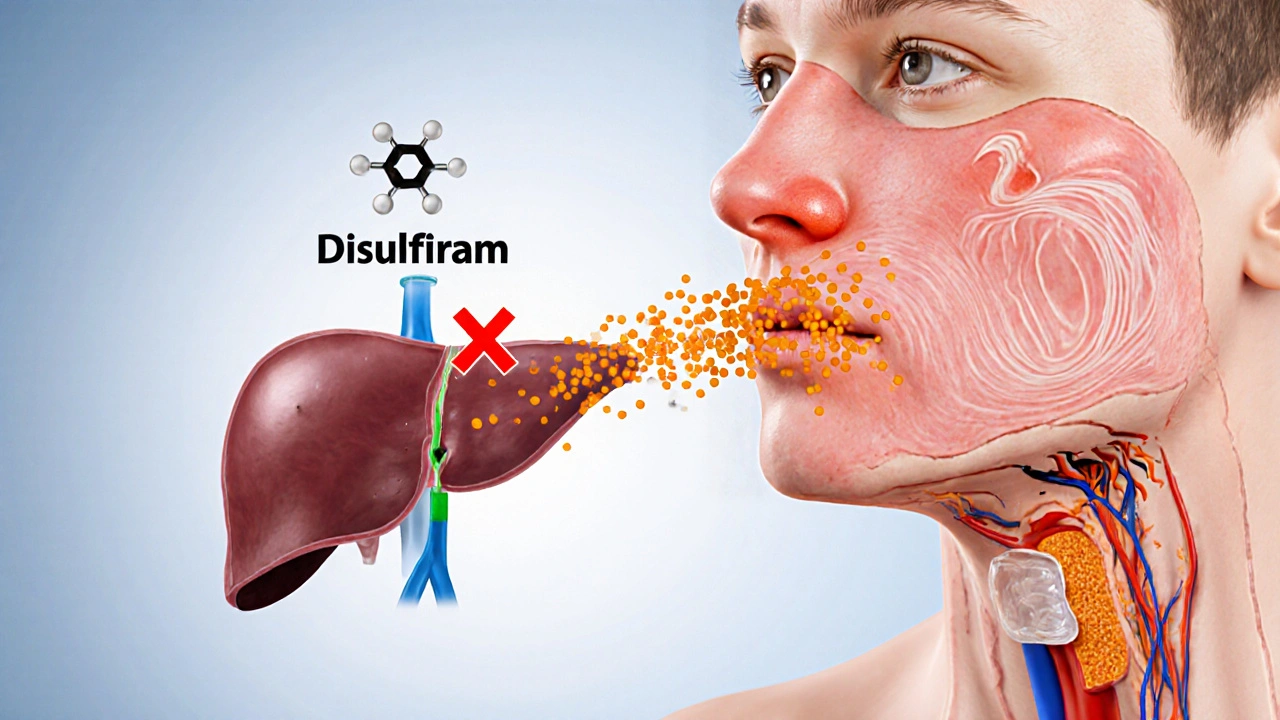
How Disulfiram Works
Disulfiram blocks the enzyme acetaldehyde dehydrogenase, causing acetaldehyde to build up when you drink. The buildup produces flushing, nausea, vomiting, and a pounding headache-an experience most people find intolerable. Because the reaction is predictable, Disulfiram is often called an “aversion therapy.”
It’s most effective for people who are highly motivated to stay completely sober and who can remember to take the pill every day. Miss a dose, and the protection disappears until you restart the medication.
Pros and Cons of Disulfiram
Pros
- Creates a strong deterrent against any alcohol consumption.
- Relatively inexpensive and widely available.
- Simple once‑daily dosing.
Cons
- Requires strict adherence; a missed dose reduces protection.
- Can cause liver toxicity (elevated liver enzymes, hepatitis) in susceptible individuals, especially when combined with alcohol.
- Side effects may include metallic taste, skin rash, and peripheral neuropathy.
- Not suitable for people with severe heart disease or psychosis.
Common Alternatives to Disulfiram
Below are the four medications most often prescribed for alcohol use disorder (AUD). Each tackles the problem from a different angle.
Naltrexone is an opioid antagonist that blocks the brain’s reward response to alcohol, reducing cravings and the pleasure of drinking. It comes in a daily tablet or a monthly injection (Vivitrol).
Acamprosate helps restore the balance of neurotransmitters disrupted by chronic alcohol use, easing post‑detox cravings is taken three times a day and is safe for people with liver impairment.
Topiramate is an anti‑seizure drug that, at lower doses, reduces the rewarding effects of alcohol and cuts cravings. It is often used off‑label for AUD.
Gabapentin is another anti‑seizure medication that can lessen anxiety and sleep disturbances during early recovery, indirectly lowering relapse risk. Like Topiramate, it is used off‑label.
Other less‑common options include Baclofen a muscle relaxant that may dampen alcohol cravings by acting on GABA‑B receptors. Research is still catching up, but some patients find it helpful.
Side‑Effect Snapshot: How the Drugs Stack Up
| Medication | Mechanism | Typical Dose | Common Side Effects | Key Contraindications | Effectiveness (Abstinence %) |
|---|---|---|---|---|---|
| Disulfiram | Acetaldehyde dehydrogenase inhibition (aversive reaction) | 250mg once daily | Flushing, nausea, headache, metallic taste, liver enzyme elevation | Severe cardiac disease, psychosis, active liver disease | ≈55‑65% |
| Naltrexone | Opioid receptor blockade (reduces reward) | 50mg daily or 380mg IM monthly | Nausea, headache, dizziness, fatigue | Acute hepatitis, opioid dependence, severe renal impairment | ≈45‑60% (higher when combined with counseling) |
| Acamprosate | Modulates glutamate & GABA balance | 666mg three times daily | Diarrhea, abdominal cramps, metallic taste | Severe renal impairment (creatinine clearance <30mL/min) | ≈40‑55% |
| Topiramate | Enhances GABA, antagonizes AMPA/kainate receptors | 25‑100mg daily (split) | Paresthesia, cognitive slowing, weight loss, taste changes | Pregnancy, severe kidney stones, uncontrolled glaucoma | ≈35‑50% (off‑label data) |
| Gabapentin | Calcium channel modulation (reduces CNS hyperexcitability) | 300‑1200mg three times daily | Drowsiness, ataxia, swelling, mood changes | Severe renal failure, hypersensitivity | ≈30‑45% (adjunct therapy) |
How to Choose the Right Medication for You
Answer these three quick questions before you talk to your doctor:
- Do you have liver disease or take other hepatotoxic drugs? If yes, steer clear of Disulfiram and consider Acamprosate or Gabapentin.
- Are you looking for a strict “no‑drink” deterrent or a craving‑reduction strategy? Disulfiram offers the former; Naltrexone focuses on the latter.
- Can you commit to daily dosing? If you struggle with pill fatigue, a monthly Naltrexone injection or a lower‑dose topiramate regimen might fit better.
Remember, medication works best when paired with counseling, support groups, or behavioral therapy. No pill can replace a solid recovery plan.

Safety Tips & Common Pitfalls
Regardless of which drug you pick, keep these safety basics in mind:
- Always disclose your full medication list-some drugs interact badly with Naltrexone or Topiramate.
- Get baseline liver function tests before starting Disulfiram or Naltrexone.
- Never drink even small amounts of alcohol while on Disulfiram; the reaction can be life‑threatening.
- Watch for signs of severe side effects (e.g., jaundice, severe headache, vision changes) and call your clinician immediately.
- Adhere to the prescribed schedule. Skipping doses reduces effectiveness and may increase relapse risk.
Real‑World Example: When Disulfiram Won’t Cut It
Mark, a 42‑year‑old accountant, started Disulfiram after a brief detox. He loved the idea of an “instant alarm” if he slipped. Within two weeks, he experienced a severe skin rash and elevated ALT/AST levels. His doctor switched him to Acamprosate, which was safe for his mild fatty liver. Mark now reports fewer cravings and no liver irritation. The lesson? Even a drug with a strong deterrent effect can backfire if your body doesn’t tolerate it.
Bottom Line
Disulfiram remains a powerful tool for those who need a hard‑stop rule, but its liver risks and adherence demands make it unsuitable for many. Naltrexone, Acamprosate, Topiramate, and Gabapentin each bring a different balance of cravings control, side‑effect profile, and dosing convenience. By matching the medication’s strengths to your health status and recovery goals, you’ll give yourself the best shot at staying sober.
Frequently Asked Questions
Can I take Disulfiram and Naltrexone together?
Combining the two is generally not recommended. Disulfiram’s aversive reaction can mask Naltrexone’s craving‑reduction effect, and both drugs strain liver function. Talk to your doctor if you’re considering a switch.
What should I do if I accidentally drink while on Disulfiram?
Seek medical attention immediately. Even a single drink can trigger a dangerous reaction, including severe vomiting, hypotension, and cardiac arrhythmias. Call emergency services if you feel faint or experience chest pain.
Is Acamprosate safe for people with kidney problems?
Acamprosate is cleared by the kidneys, so severe renal impairment (creatinine clearance <30mL/min) is a contraindication. Dose adjustments may be possible for moderate impairment, but a nephrologist’s input is essential.
How long do I need to stay on medication after I stop drinking?
Most guidelines suggest a minimum of six months to a year, depending on the drug and your relapse risk. Long‑term maintenance (2‑3years or more) can be beneficial for high‑risk individuals, especially with Naltrexone or Acamprosate.
Can I use these medications if I’m pregnant?
Pregnancy is a red flag for most AUD drugs. Disulfiram, Naltrexone, and Topiramate are generally contraindicated. Acamprosate may be considered in rare cases, but only under specialist supervision.





Comments
Alex EL Shaar
October 10, 2025 AT 22:31 PMYo, the Disulfiram thing is like a nasty hangover on steroids, mate. If you skip a pill, it's basically a free pass for the next binge, which is a huge risk for folks who *can’t* remember to pop it daily. The liver toxicity stuff? Yeah, that’s a legit concern – especially if you’re already tip‑toeing around elevated enzymes. In my experience, the cheap price tag is the only thing that keeps people from ditching the med, but the side‑effects list reads like a horror movie script. Flushing, metallic taste, neuropathy – not exactly a party trick. Also, the aversive reaction only works if you *actually* drink, so total abstainers might feel like they’ve wasted a pill. Bottom line: Disulfiram is a blunt‑tool for the ultra‑motivated, not a catch‑all solution.
Anna Frerker
October 15, 2025 AT 13:38 PMDisulfiram is a harsh wake‑up call.
Edward Morrow
October 20, 2025 AT 04:44 AMListen up, the whole “make alcohol taste terrible” gimmick is a double‑edged sword. Sure, it scares the hell out of you if you sip, but it also turns you into a ticking time bomb for liver damage if you ever slip up. The medicine forces you to stay disciplined, which is great for the iron‑willed, but anyone with a shaky routine will find the protection evaporating quicker than cheap vodka at a college party. And don’t forget the psychosomatic side‑effects – metallic tongue, skin rash, neuropathy – they can be just as debilitating as the hangover you’re trying to avoid. If you’re already dealing with cardiac issues or psychosis, you’re basically signing up for a medical disaster. Bottom line: Antabuse isn’t a magic bullet; it’s a harsh deterrent that only works for the truly committed.
Shayne Tremblay
October 24, 2025 AT 19:51 PMHey everyone! If you’re looking for a medication that won’t drain your wallet and can really keep you on track, Disulfiram can be a solid choice – just make sure you’re ready for the daily commitment. Pair it with counseling or a support group, and you’ll see the best results. Remember, staying sober is a team sport – meds are just one player on the field.
Stephen Richter
October 29, 2025 AT 09:58 AMIt must be noted that the use of Disulfiram carries significant contraindications, notably severe cardiac disease and active hepatic pathology. Patients should undergo thorough screening before initiation.
Musa Bwanali
November 3, 2025 AT 01:04 AMAlright, let’s get real – if you’re committed to quitting, Disulfiram can be a powerful ally, but only if you’re consistent. Miss a dose and you lose the safety net. Combine it with proper therapy and you’ll maximize those abstinence numbers.
Allison Sprague
November 7, 2025 AT 16:11 PMFirst off, the grammar in the “side‑effect snapshot” table is riddled with inconsistencies – “Flushing, nausea, headache” versus “Nausea, headache, dizziness” – the lack of parallel structure is glaring. Also, the phrase “high liver toxicity” is vague; specify enzyme elevation ranges for clarity. Finally, the article jumps from mechanism to pros/cons without transitional sentences, making it feel disjointed.
leo calzoni
November 12, 2025 AT 07:18 AMDisulfiram is quite the blunt instrument; it forces an aversive reaction that deters drinking. However, its reliance on perfect adherence limits its practicality for many patients.
KaCee Weber
November 16, 2025 AT 22:24 PMOkay, let’s unpack this whole medication maze step by step, because there’s a lot to consider and I want to make sure we don’t miss any nuance. First, Disulfiram works by blocking acetaldehyde dehydrogenase, which causes a build‑up of acetaldehyde when alcohol is consumed, leading to an intense flushing, nausea, vomiting, and headache experience that most people find intolerable – essentially turning any drink into a nightmare scenario. This mechanism is very clear and straightforward, but it also means that you have to be 100 % compliant; miss a dose and the protective barrier disappears, which can be a huge risk for anyone with a chaotic daily routine. In contrast, Naltrexone acts as an opioid antagonist, reducing the rewarding feeling of alcohol and thereby lowering cravings; it can be taken daily or as a monthly injection, which some patients find more convenient, though you need to be abstinent before starting it to avoid precipitating withdrawal. Acamprosate, on the other hand, stabilizes the glutamate‑GABA system after detox and is taken three times a day; it’s especially useful for people with liver issues because it’s renally excreted, but the three‑times‑daily dosing can be a compliance hurdle. Then there are the off‑label anti‑seizure medications like Topiramate and Gabapentin. Topiramate can reduce cravings at lower doses but comes with cognitive side effects such as confusion and memory problems, while Gabapentin is more about easing anxiety and sleep disturbances, which indirectly helps maintain sobriety. Baclofen, a muscle relaxant that works on GABA‑B receptors, shows promise in some studies for reducing cravings, yet the evidence base is still thin and side‑effects like drowsiness are common. Aside from efficacy, the side‑effect profiles vary dramatically: Disulfiram has a high side‑effect burden, especially liver toxicity, whereas Naltrexone’s side effects are generally low but can include nausea and dizziness; Acamprosate is well‑tolerated but can cause diarrhea. In terms of cost, Disulfiram is the cheapest, which is a plus for patients without insurance, while the injectable form of Naltrexone (Vivitrol) can be quite pricey. Ultimately, the choice depends on your liver health, your ability to stick to a dosing schedule, and whether you need something that blocks cravings or one that creates a deterrent effect. 💊✨🚀
kristina b
November 21, 2025 AT 13:31 PMWhen contemplating the pharmacologic armamentarium for alcohol use disorder, one must adopt a holistic perspective that transcends mere efficacy percentages. While Disulfiram’s aversive conditioning offers a stark deterrent, it simultaneously imposes an onerous demand for unwavering adherence, lest the protective veil be lifted and the patient be exposed to the dreaded acetaldehyde surge. Contrastingly, Naltrexone, with its opioid receptor antagonism, attenuates the hedonic reinforcement of ethanol, fostering a more subtle yet sustained attenuation of craving. Yet, this subtlety is not without caveats: the necessity for pre‑treatment abstinence and the specter of hepatotoxicity in vulnerable individuals demand vigilant monitoring. Acamprosate, by modulating the glutamatergic‑GABAergic equilibrium, addresses the neurochemical chaos persisting post‑detox, rendering it a valuable ally for maintaining sobriety, particularly in those burdened with hepatic compromise. Off‑label agents such as Topiramate and Gabapentin, though promising, introduce cognitive and sensory side‑effects that may erode compliance. In the final analysis, the optimal therapeutic strategy must be individualized, integrating patient motivation, comorbidities, and psychosocial supports, thereby transforming pharmacotherapy from a blunt instrument into a finely tuned instrument of recovery.
Ida Sakina
November 26, 2025 AT 04:38 AMIt is incumbent upon clinicians to weigh the ethical implications of prescribing an agent that induces deliberate physiological distress upon alcohol ingestion. The principle of non‑maleficence must be reconciled with the potential beneficence derived from the medication's deterrent effect. Moreover, informed consent should encompass a thorough exposition of hepatic ramifications, neuropathic sequelae, and dermatologic manifestations. Such transparency ensures that patients are not merely passive recipients but active participants in their therapeutic odyssey.
Amreesh Tyagi
November 30, 2025 AT 19:44 PMi think disulfiram is overrated you can just avoid drinking no need for meds
Robert Jaskowiak
December 5, 2025 AT 10:51 AMHonestly, meds are just a crutch if you aren’t willing to confront the underlying issues. Disulfiram can be useful, sure, but it won’t fix a broken mindset. Pair it with therapy or you’re just playing roulette.
Vic Harry
December 10, 2025 AT 01:58 AMDisulfiram is just a cheap way to scare people off drinking it works but you gotta be consistent
Suman Wagle
December 14, 2025 AT 17:04 PMWell, while some folks think you can just ‘willpower’ your way out, the data shows a combination of pharmacotherapy and supportive counseling yields the highest abstinence rates; ignoring the science is a disservice to anyone truly trying to recover.
Neil Sheppeck
December 19, 2025 AT 08:11 AMIt’s fascinating how each medication targets a different neuro‑biological pathway, and that’s why a personalized approach-considering liver function, dosing convenience, and side‑effect tolerability-makes the biggest difference in long‑term success.